If I had to choose a single topic as the most absolutely important one that everybody who works with patients and families facing advanced illness and end of life needs to fully understand and appreciate, it would have to be delirium.
If I had to identify the single greatest concern shared by every patient and family we meet, my bet would still be on delirium. When we know delirium, we can help. If we don't, we're going to fly that plane right into the ground.
No other topic comes close to delirium in exposing the gaps in our knowledge and the deficiencies in our practice. That is as true today as it was 27 (!) years ago, when Sharon Inouye and colleagues first developed the Confusion Assessment Method (CAM) to help non-psychiatric clinicians practicing in high-risk settings identify and manage delirium:
“Delirium is often overlooked, misdiagnosed as depression or psychosis, or misattributed to dementia or senescence. In one study, 32% of cases went unrecognized by physicians.” 1
What about nurses’ understanding and effectiveness regarding delirium?
It only takes a few minutes with Google and the search phrase, “nurses understanding and effectiveness regarding delirium,” to start gathering evidence:
“A lack of education and general ignorance of delirium, in particular about the benefits of early recognition and treating delirium, emerged as a strong barrier ... as a consequence of a superficial teaching about delirium during medical or nursing studies.” 2
Where should we start?
I developed an in-service program on assessing and managing delirium a few years ago. I also tried to summarize the material in a ‘Top 5’ list, highlighting the essential points every hospice clinician should know.
Maybe we can start with a simple question: How prevalent is delirium?
The answer depends on where you look.
Let’s screen 100 people for delirium in different health care settings. The incidence of delirium in these illustrations is based on multiple sources, and varies by source. Here’s one you can check. 3 You may find the numbers I use too high, or too low. I think the exact figures are less important than the general trend.
First, let's say hello to our friendly 100:
If I had to identify the single greatest concern shared by every patient and family we meet, my bet would still be on delirium. When we know delirium, we can help. If we don't, we're going to fly that plane right into the ground.
No other topic comes close to delirium in exposing the gaps in our knowledge and the deficiencies in our practice. That is as true today as it was 27 (!) years ago, when Sharon Inouye and colleagues first developed the Confusion Assessment Method (CAM) to help non-psychiatric clinicians practicing in high-risk settings identify and manage delirium:
“Delirium is often overlooked, misdiagnosed as depression or psychosis, or misattributed to dementia or senescence. In one study, 32% of cases went unrecognized by physicians.” 1
What about nurses’ understanding and effectiveness regarding delirium?
It only takes a few minutes with Google and the search phrase, “nurses understanding and effectiveness regarding delirium,” to start gathering evidence:
“A lack of education and general ignorance of delirium, in particular about the benefits of early recognition and treating delirium, emerged as a strong barrier ... as a consequence of a superficial teaching about delirium during medical or nursing studies.” 2
Where should we start?
I developed an in-service program on assessing and managing delirium a few years ago. I also tried to summarize the material in a ‘Top 5’ list, highlighting the essential points every hospice clinician should know.
Maybe we can start with a simple question: How prevalent is delirium?
The answer depends on where you look.
Let’s screen 100 people for delirium in different health care settings. The incidence of delirium in these illustrations is based on multiple sources, and varies by source. Here’s one you can check. 3 You may find the numbers I use too high, or too low. I think the exact figures are less important than the general trend.
First, let's say hello to our friendly 100:
When we screen for delirium in the community, assessing our 100 while they’re out on their daily business, we’d find about this many delirious:
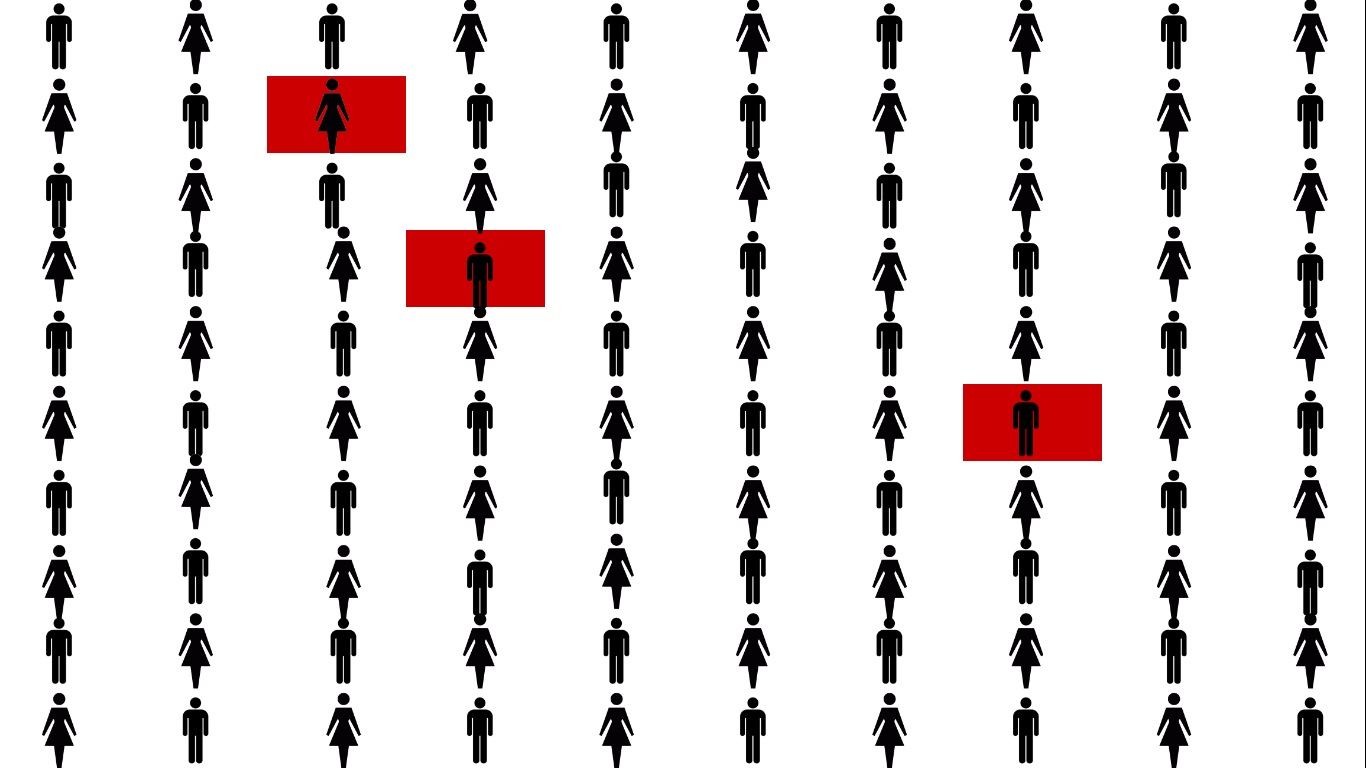
That's about 3%, much of it because of intoxication or withdrawal.
When we go to the hospital, this is what we find:
When we go to the hospital, this is what we find:
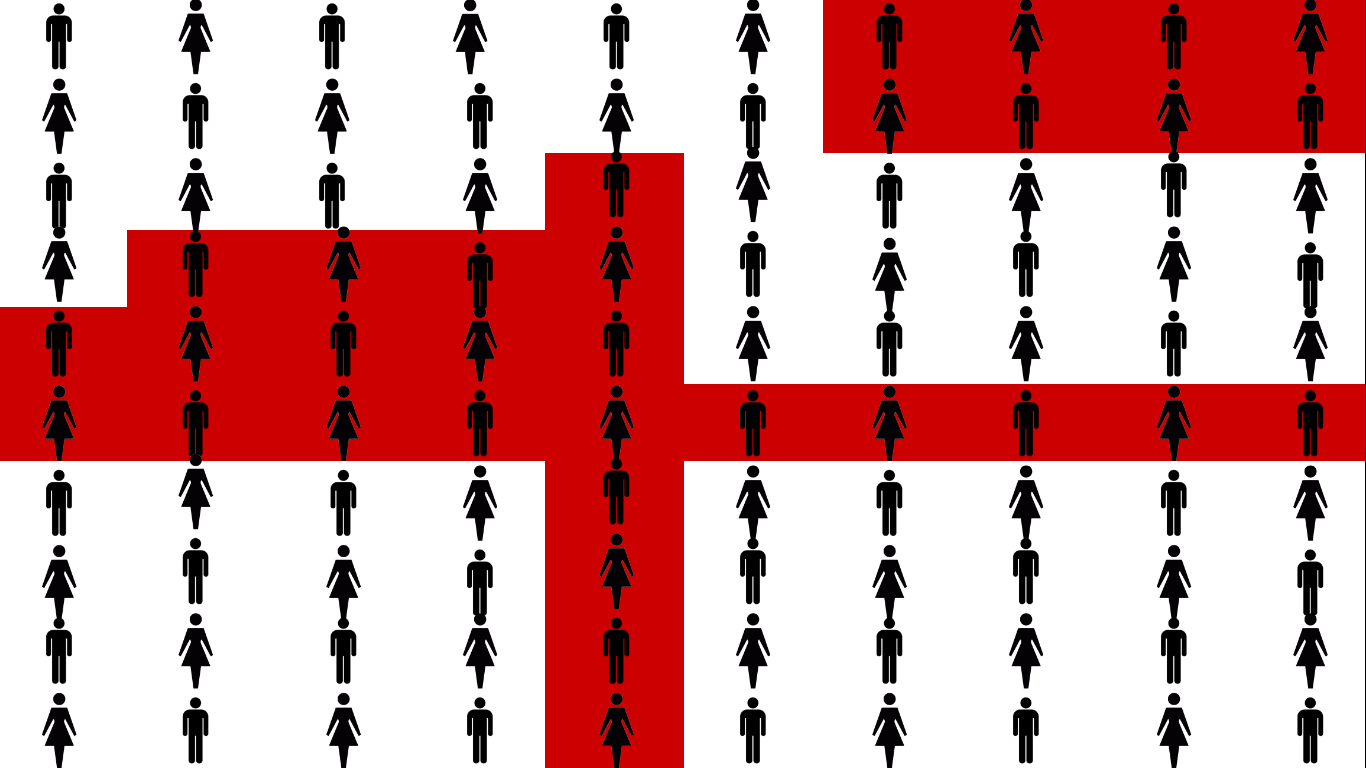
About 1/3 of a hospital's population lives in red. That’s a lot, but it makes sense, since hospital inpatients are sick or injured, both of which are significant risk factors for developing delirium.
Not everyone is delirious at the same time. Some are admitted in a state of delirium (quick question - what’s the #1 reason for ER visits by the elderly?), others develop delirium during their stay but it’s resolved before discharge, while others are still delirious when they're discharged home or to a facility.
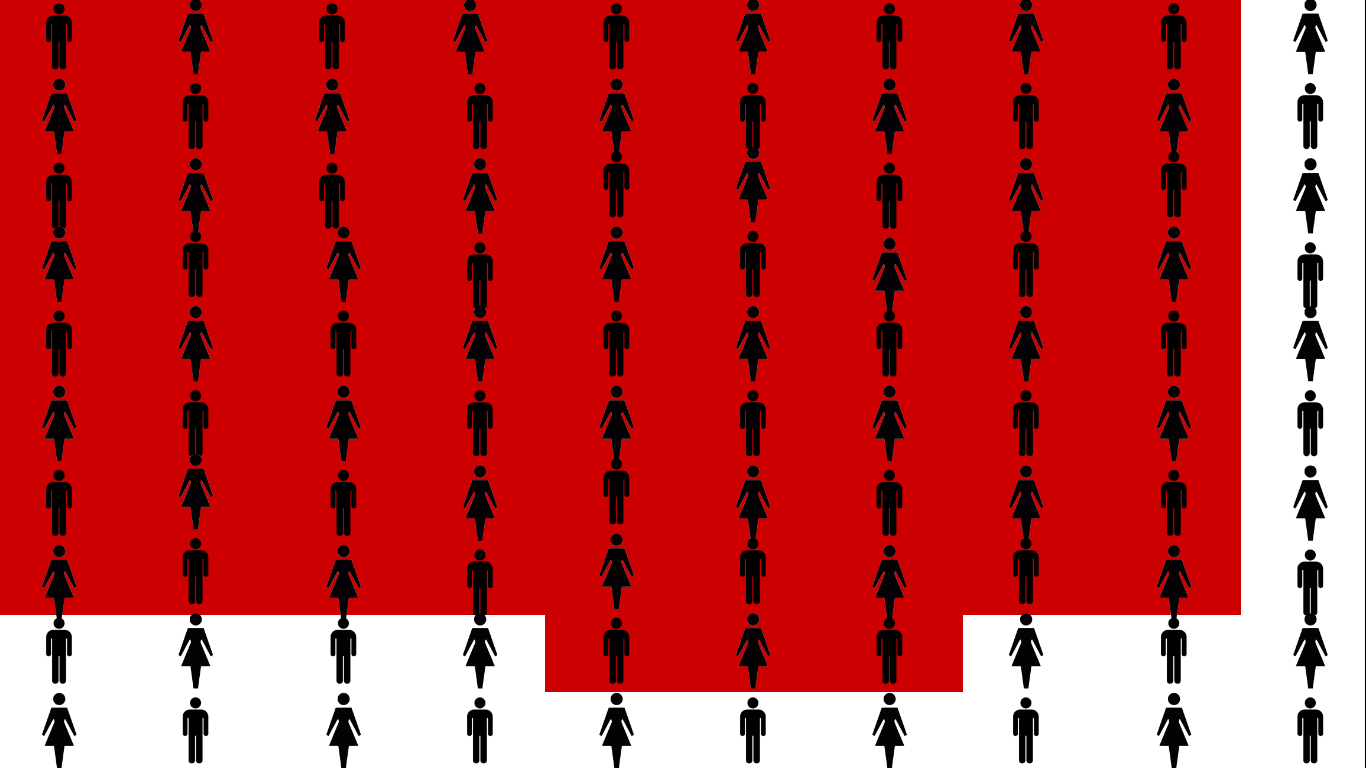
Let’s assess the group in a facility, specifically a skilled nursing and rehabilitation center for people who require additional care and treatment, like following a hip replacement.
Not everyone is delirious at the same time. Some are admitted in a state of delirium (quick question - what’s the #1 reason for ER visits by the elderly?), others develop delirium during their stay but it’s resolved before discharge, while others are still delirious when they're discharged home or to a facility.
Let’s assess the group in a facility, specifically a skilled nursing and rehabilitation center for people who require additional care and treatment, like following a hip replacement.
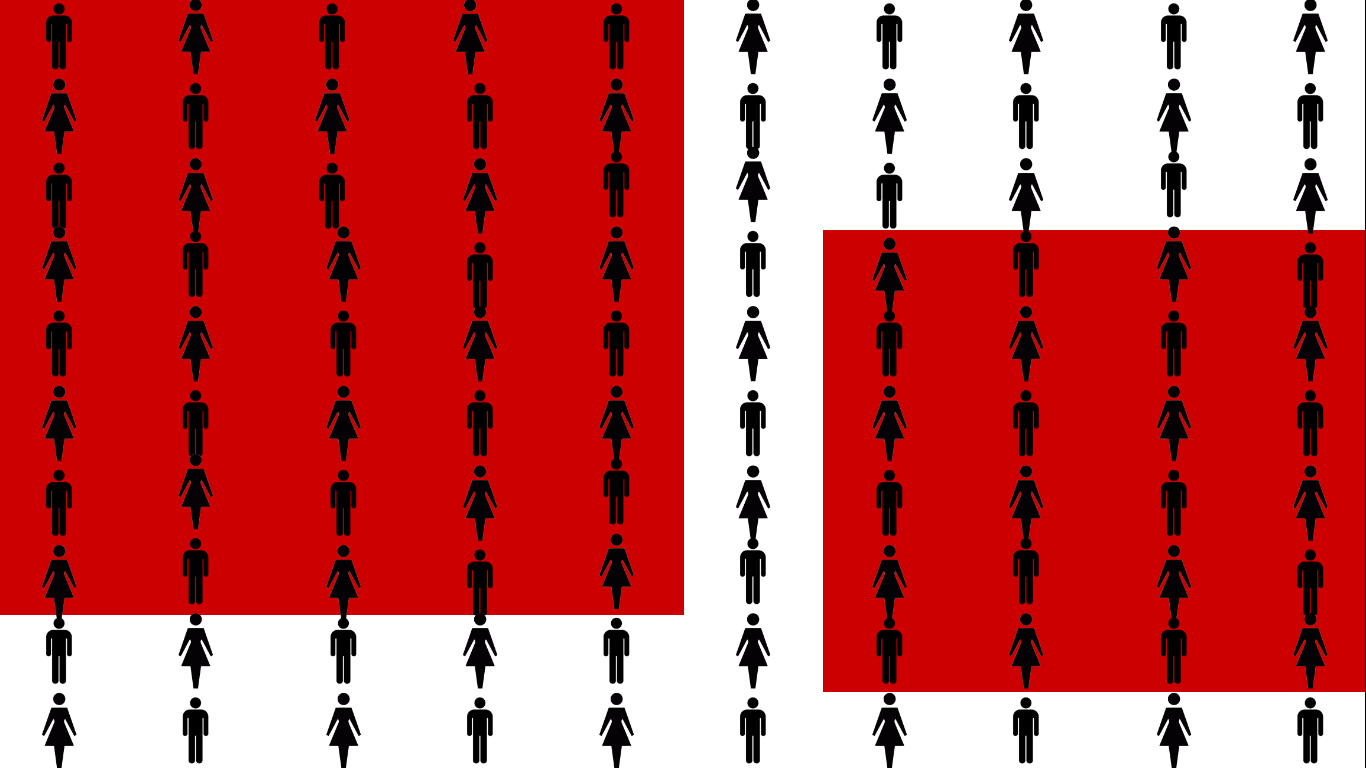
That’s 2/3, a clear majority! Why? People are transferred here from the hospital, where about a third develop delirium, including those who were still delirious when they were discharged.
This group also skews older, a significant risk factor for delirium. People also stay here longer, increasing their opportunities for repeated and prolonged exposure to additional risk factors, like sensory overload or deprivation, disrupted sleep, polypharmacy, and time.
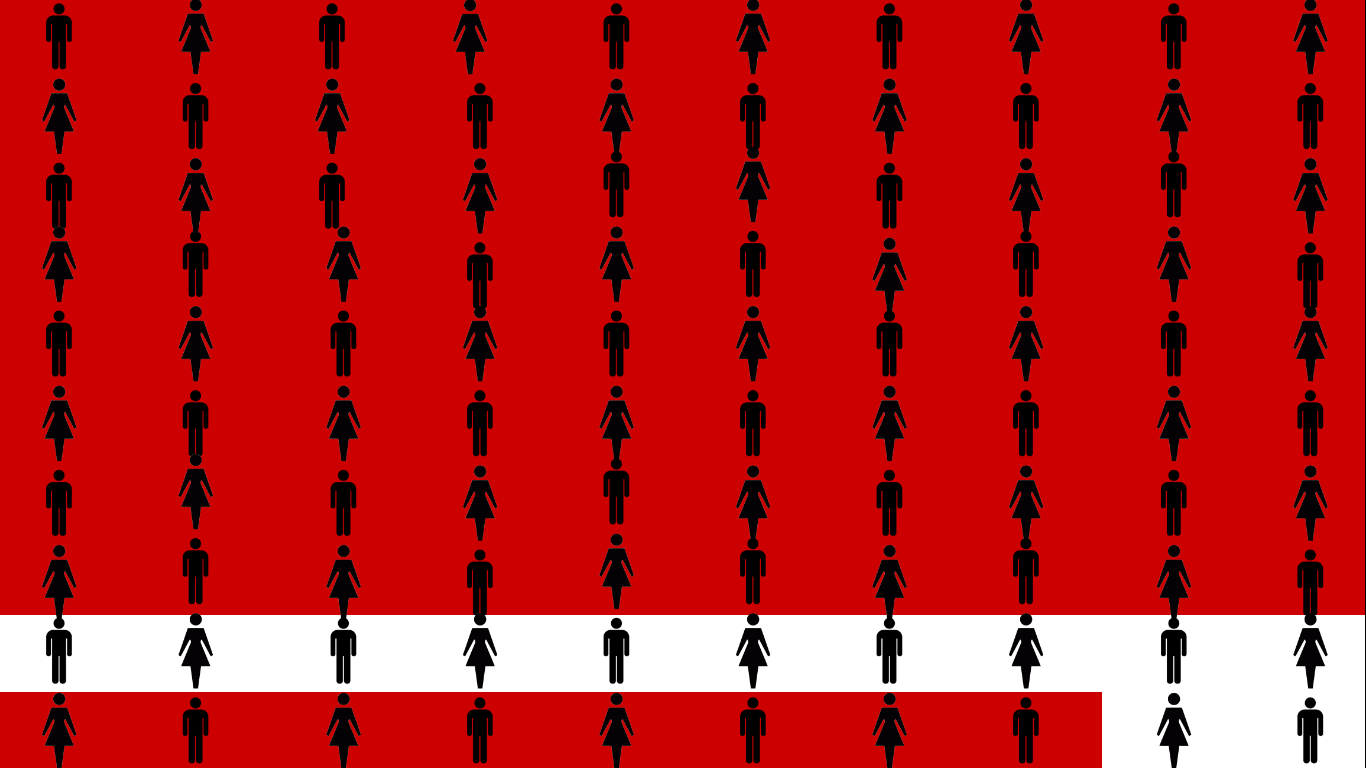
Our next stop is the intensive care unit (ICU).
This group also skews older, a significant risk factor for delirium. People also stay here longer, increasing their opportunities for repeated and prolonged exposure to additional risk factors, like sensory overload or deprivation, disrupted sleep, polypharmacy, and time.
Our next stop is the intensive care unit (ICU).
Delirium affects 75% of these, the sickest of the sick, because they’re given the most, and most powerful, medications, and are cared for in the most abnormal and disruptive setting of all.
There’s one last place for us to explore - end of life.
Which brings us to our Top 5 list of things every hospice clinician should know about delirium:
#5 - Expect delirium in every hospice patient. Delirium is a medical emergency. Over 85% of people at end of life experience delirium, so assume delirium is present until your assessment proves otherwise. Delirium is a deeply distressing symptom for patients and families. It undermines important goals at end of life, including comfort and meaningful interaction with family. 4, 5
***
- Inouye, S. et al. Clarifying Confusion: The Confusion Assessment Method. Annals of Internal Medicine. 1990;113:941-948.
- Andrew Teodorczuk, A. Reynish, E. Milisen, K. Improving recognition of delirium in clinical practice: a call for action. BMC Geriatrics 2012 12:55 DOI: 10.1186/1471-2318-12-55.
- Vasilevskis, E. Han, J. Hughes, C. Ely, E. Epidemiology and risk factors for delirium across hospital settings. Best Pract Res Clin Anaesthesiol. 2012 September; 26(3): 277–287. doi:10.1016/j.bpa.2012.07.003.
- Ganzini, L. Care of patients with delirium at end of life. Annals of Long Term Care. 2007;15(3)
- Szarpa, K. et al. Prodrome to delirium, a grounded theory study. Journ Hospice Palliative Nsg. 2013; 15(6):332-337.