If you work in hospice, and someone asks you about it, what's a good way to respond?
If you know nothing about hospice, but wonder about it sometimes, where can you go to find out more?
If you've had an experience with hospice, and wonder about other people's, how can you compare?
I think the answer to these and other questions starts with a visit to the websites* of award-winning photographer Ross Taylor, for his 2002 photo essay, "Gloria's Goodbye."
From his introduction:
"One night, while she was getting treatment, Gloria looked up to me and told me how much she cared about me, and how much doing this story meant to her. We both cried alone in her bedroom; it is a moment I will never forget. I always want people to know this part of her tenderness when seeing these images, especially the ones around her decline and death.”
Blog sez check it out.
Gloria's Goodbye
* Taylor has both a dot com and a dot net, and there seems to be a slight difference in the versions of the story. I like the one at the dot net site.
Wednesday, May 17, 2017
Monday, May 8, 2017
Something else about delirium, part 2
It's Number One!!
Every clinician working with patients and families facing advanced illness and at end of life must understand delirium. We already know to expect it, because that’s #5 on the Top 5 List.
Delirium, dementia, and depressions, “the 3Ds,” are frequently encountered in life-limiting illness and at end of life. Older patients are particularly vulnerable. A recent study found that nurses had generally low knowledge of the 3Ds, and were not able to effectively identify, differentiate, or intervene when one or more of the disorders affected their patients. 1
The clinical presentation of delirium varies widely. While many clinicians most often think of delirium as a state of extreme agitation and hyperactivity, the hypoactive and mixed forms of delirium occur more frequently in older patients. 2
It’s possible to spend hours, days, weeks, or an entire career exploring a specific topic like delirium.
Thankfully, it’s also possible to learn the essentials much more quickly. The folks at PC NOW (the Palliative Care Network of Wisconsin) produce Palliative Care Fast Facts and Concepts.
I’ve been lucky to work with physicians who understand palliative care and hospice, but if any at your agency need to be brought up to speed on any topic, grab this link and make sure they do something with it. It could be the most important contribution you ever make to good care.
#4 - Know what delirium is. A simple definition says it best - delirium is present when, “a patient’s ability to receive, process, store, and recall information is impaired.” 3
***
- Yaghmour, S.M. and Gholizadeh, L. (2016) Review of Nurses’ Knowledge of Delirium, Dementia and Depressions (3Ds): Systematic Literature Review. Open Journal of Nursing, 6, 193-203.
- Weissman, D. Rosielle, D. Fast Facts and Concepts #1: Diagnosis and Treatment of Terminal Delirium. 3rd Rev. November, 2014. Downloaded at https://www.mypcnow.org/blank-qbv4q
- Ely, W. et al. Confusion Assessment Method for the ICU - Training Manual. Rev. 2014. Available at http://www.icudelirium.org/
Friday, May 5, 2017
Sing it to me

illustration by ahna jin
I just delivered another script to Adam, the fellow I met on Fiverr who is doing the voiceover work for a series of instructional videos on caring for patients and families with advanced dementia at end of life.
This latest installment explores ways to connect with someone when their cognition is absent, or severely compromised.
We often fail to appreciate how normal cognitive interaction is no longer possible for someone with advanced dementia, like having a conversation based on questions and recollections.
Writing for TheAlzheimersSite, Elizabeth Nelson likewise details the consequences of our failure to adapt to the needs of those with dementia in its earlier stages.
I’m working with an artist to help inform the video’s content and convey the stories more effectively. We want the material to have the look and feel of a children’s book, to put people more at ease in the face of what can be an emotional and difficult topic. The image above is our attempt to express the idea of advanced dementia realistically, but also in a way that is less threatening or disturbing.
Singing is one reliable way to connect with someone who has advanced dementia, and for some reason when we do, we often reach for, “You are my sunshine.”
The melody can be soothing or spirited, but the lyrics are always heartbreaking. Here’s a version that really floored me.
Tuesday, May 2, 2017
Would YOU attend this in-service?
I’ve been working on some educational content for an agency that cares for patients and families with advanced dementia, in response to regulations from the Massachusetts Department of Public Health requiring eight hours of dementia-specific staff training.
As these folks helpfully explain, “Previously, nursing homes and other facilities were technically permitted to advertise their services as specializing in dementia care, even though their staffs were not appropriately trained…”
Ahem.
Jeanne had a mantra about teaching that was the foundation for everything she tried to do in classroom and clinical settings:
“Mediocre teachers convey information. Adequate teachers provoke discussion. Outstanding teachers inspire.”
My project colleagues and I have explored different ways to develop, package, and present the material. Our goal is to enhance skills and understanding, and support the kinds of sustainable positive changes in staff behavior that lead to higher quality service, and result in better outcomes for patients and families.
Videos are an important part of our model.
I’ve been critical of what passes for “continuing education” in health care for about as long as I’ve been a nurse, because I’ve been forced to endure more crappy programs and “death by PowerPoint” than I can count.
I’ve tried watching in-house videos with low production values featuring presenters more suited to print, or who would benefit from simple coaching. But it usually takes just a minute or two for me to want to jab large knitting needles into my eyeballs.
Maybe I’m too sensitive.
We plan to award contact hours to the nurses who attend these programs, so I’ve also been working on the detailed application for approval by our state ANA chapter. The application guidelines include specific language required to disclose information about earning credit, along with any conflicts of interest or commercial support.
I first recorded my own narration for this and the other video elements, but still wanted to reach for the knitting needles. I thought a woman’s voice, speaking with a British accent, would be much better.
Someone told me about Fiverr, where I found the perfect person (voice).
I told a friend about my plan. She replied, “Use a man’s voice,” and made a compelling case that quickly won me over.
Here’s a version of what will be included at the start of each video, once they’ve been approved to award nursing contact hours. I think my friend was right.
Monday, May 1, 2017
A death I nursed

Jeanne at Carlisle Pines State Forest (MA), 2014
The nurse educator with the biggest influence on my personal and professional life was Jeanne, the nurse educator I married.
The first serious discussion we ever had was about death.
One Saturday night in early October, 1975, my best friend’s father died suddenly at home. Jeanne was the head of my third-year nursing program, and on Monday I told her I would be absent for the rest of the week, missing three full clinical days as well as another day of class.
It was right at the start of a full curriculum in a tight schedule, and I expected her to object. But instead, Jeanne listened, asked what else I needed, and said not to worry, that we’d find a way to make up the lost time.
One year later, my casual visit to the school as a newly-minted RN led to more conversations and, later, a date to watch the Boston Ballet. Things happened, and we married in 1981.
Fast forward to January, 2016 - our final approach to Jeanne’s end of life after five years of Alzheimer’s. Here was the time to apply everything I ever learned in classes and clinical settings.
We often talked about death in those intervening years. Not morbidly or obsessively, but simply because we shared a profession and benefitted from each other’s perspective.
We supported each other as we lost family members and friends, and made sure to say, “Please, don’t ever do this to me when I die!” whenever we saw something we didn’t want for ourselves - embalming and an open casket, a funeral in a church, a line of limos in a crowded cemetery by a busy highway, dove-shaped balloons, tension.
We had conversations about advanced disease and our preferences for care - usually in the context of someone else’s illness, and again often provoked by what we saw, personally and professionally. “Please don’t let them do this to me if I’m ever that sick!”
Our plan of care in Jeanne’s final years was straightforward, with simple goals based entirely on what was important to her, and on what she wanted: to be safe, comfortable, and content at home, where she could be dignified and loved.
We met our goals.
It was the last, most critical test we ever faced. I can’t remember if it was easy or hard. We were just trying to make the best of a bad situation. But for me, as was the case in all the rest of our lives together, it was really a matter of keeping up with Jeanne.
Friday, April 28, 2017
Something about delirium, part 1
If I had to choose a single topic as the most absolutely important one that everybody who works with patients and families facing advanced illness and end of life needs to fully understand and appreciate, it would have to be delirium.
If I had to identify the single greatest concern shared by every patient and family we meet, my bet would still be on delirium. When we know delirium, we can help. If we don't, we're going to fly that plane right into the ground.
No other topic comes close to delirium in exposing the gaps in our knowledge and the deficiencies in our practice. That is as true today as it was 27 (!) years ago, when Sharon Inouye and colleagues first developed the Confusion Assessment Method (CAM) to help non-psychiatric clinicians practicing in high-risk settings identify and manage delirium:
“Delirium is often overlooked, misdiagnosed as depression or psychosis, or misattributed to dementia or senescence. In one study, 32% of cases went unrecognized by physicians.” 1
What about nurses’ understanding and effectiveness regarding delirium?
It only takes a few minutes with Google and the search phrase, “nurses understanding and effectiveness regarding delirium,” to start gathering evidence:
“A lack of education and general ignorance of delirium, in particular about the benefits of early recognition and treating delirium, emerged as a strong barrier ... as a consequence of a superficial teaching about delirium during medical or nursing studies.” 2
Where should we start?
I developed an in-service program on assessing and managing delirium a few years ago. I also tried to summarize the material in a ‘Top 5’ list, highlighting the essential points every hospice clinician should know.
Maybe we can start with a simple question: How prevalent is delirium?
The answer depends on where you look.
Let’s screen 100 people for delirium in different health care settings. The incidence of delirium in these illustrations is based on multiple sources, and varies by source. Here’s one you can check. 3 You may find the numbers I use too high, or too low. I think the exact figures are less important than the general trend.
First, let's say hello to our friendly 100:
If I had to identify the single greatest concern shared by every patient and family we meet, my bet would still be on delirium. When we know delirium, we can help. If we don't, we're going to fly that plane right into the ground.
No other topic comes close to delirium in exposing the gaps in our knowledge and the deficiencies in our practice. That is as true today as it was 27 (!) years ago, when Sharon Inouye and colleagues first developed the Confusion Assessment Method (CAM) to help non-psychiatric clinicians practicing in high-risk settings identify and manage delirium:
“Delirium is often overlooked, misdiagnosed as depression or psychosis, or misattributed to dementia or senescence. In one study, 32% of cases went unrecognized by physicians.” 1
What about nurses’ understanding and effectiveness regarding delirium?
It only takes a few minutes with Google and the search phrase, “nurses understanding and effectiveness regarding delirium,” to start gathering evidence:
“A lack of education and general ignorance of delirium, in particular about the benefits of early recognition and treating delirium, emerged as a strong barrier ... as a consequence of a superficial teaching about delirium during medical or nursing studies.” 2
Where should we start?
I developed an in-service program on assessing and managing delirium a few years ago. I also tried to summarize the material in a ‘Top 5’ list, highlighting the essential points every hospice clinician should know.
Maybe we can start with a simple question: How prevalent is delirium?
The answer depends on where you look.
Let’s screen 100 people for delirium in different health care settings. The incidence of delirium in these illustrations is based on multiple sources, and varies by source. Here’s one you can check. 3 You may find the numbers I use too high, or too low. I think the exact figures are less important than the general trend.
First, let's say hello to our friendly 100:
When we screen for delirium in the community, assessing our 100 while they’re out on their daily business, we’d find about this many delirious:
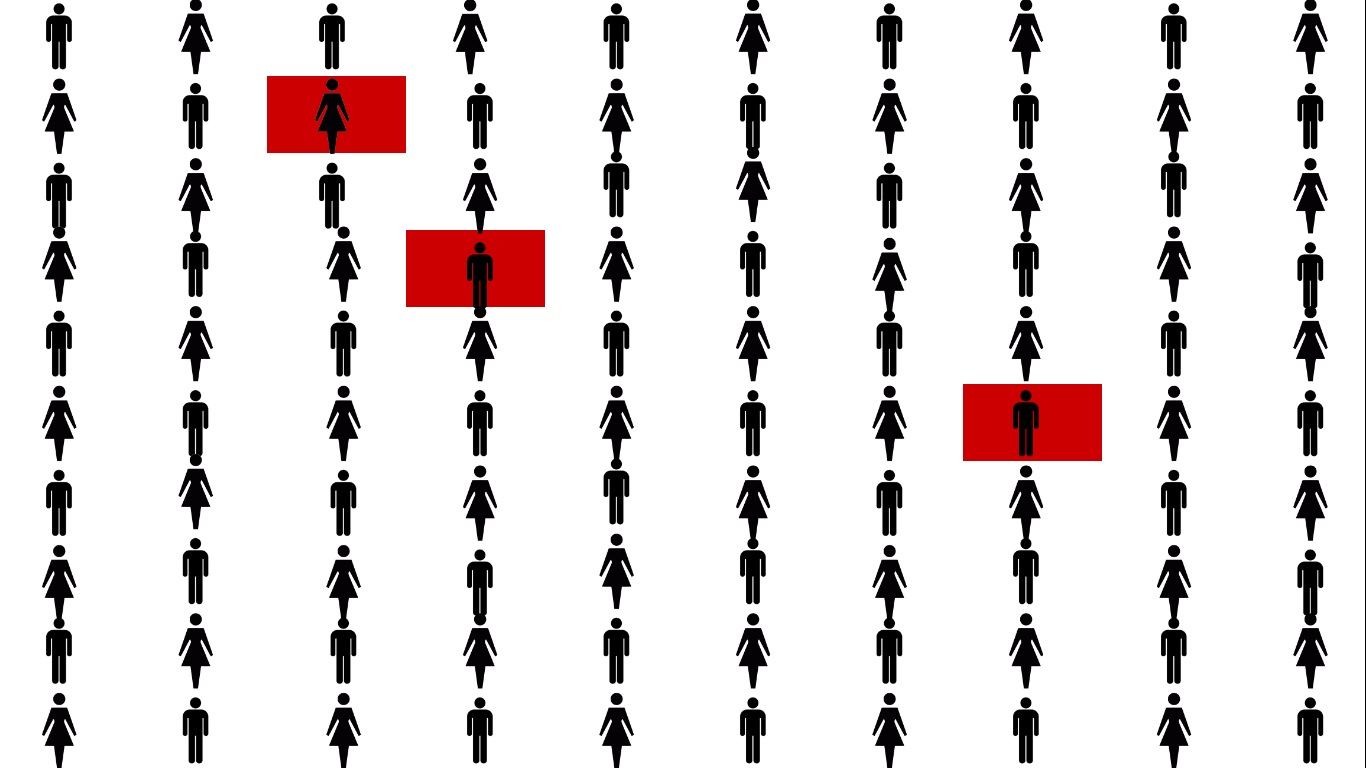
That's about 3%, much of it because of intoxication or withdrawal.
When we go to the hospital, this is what we find:
When we go to the hospital, this is what we find:
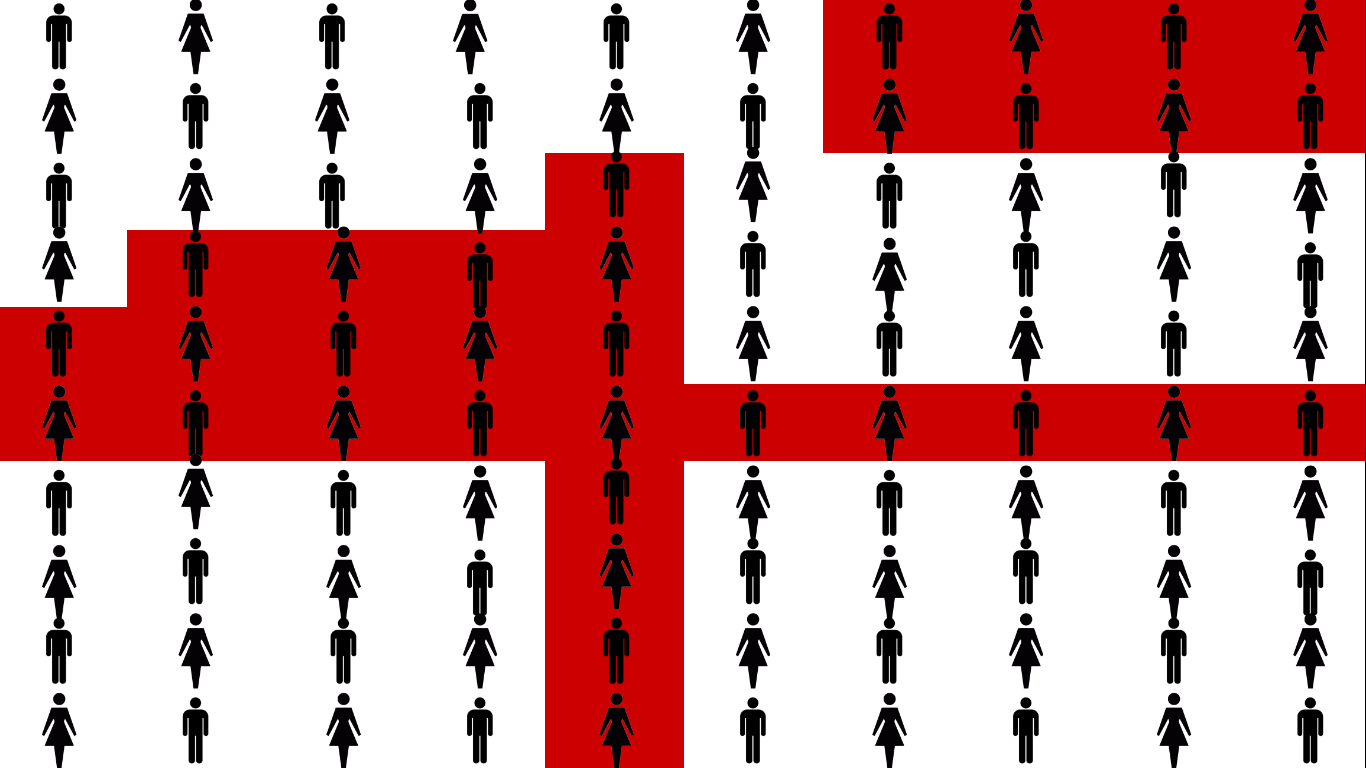
About 1/3 of a hospital's population lives in red. That’s a lot, but it makes sense, since hospital inpatients are sick or injured, both of which are significant risk factors for developing delirium.
Not everyone is delirious at the same time. Some are admitted in a state of delirium (quick question - what’s the #1 reason for ER visits by the elderly?), others develop delirium during their stay but it’s resolved before discharge, while others are still delirious when they're discharged home or to a facility.
Let’s assess the group in a facility, specifically a skilled nursing and rehabilitation center for people who require additional care and treatment, like following a hip replacement.
Not everyone is delirious at the same time. Some are admitted in a state of delirium (quick question - what’s the #1 reason for ER visits by the elderly?), others develop delirium during their stay but it’s resolved before discharge, while others are still delirious when they're discharged home or to a facility.
Let’s assess the group in a facility, specifically a skilled nursing and rehabilitation center for people who require additional care and treatment, like following a hip replacement.
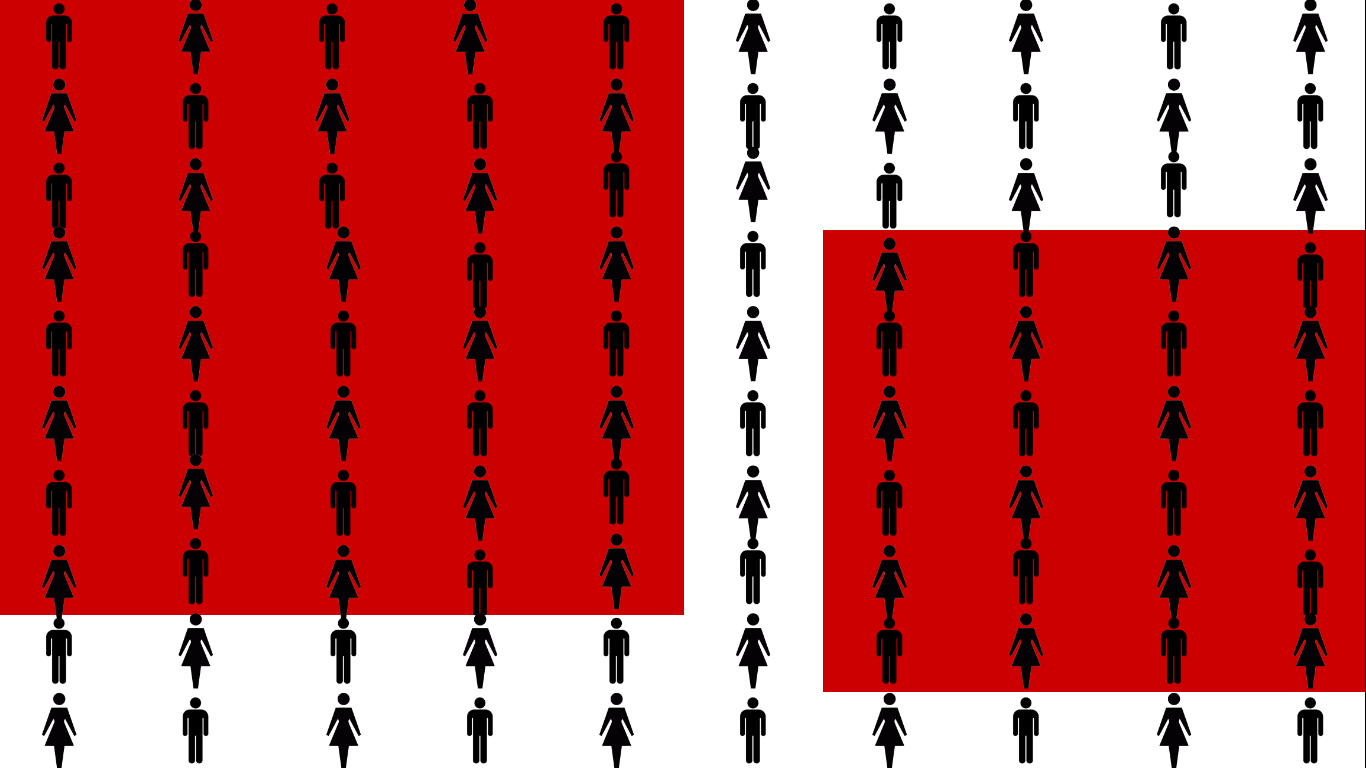
That’s 2/3, a clear majority! Why? People are transferred here from the hospital, where about a third develop delirium, including those who were still delirious when they were discharged.
This group also skews older, a significant risk factor for delirium. People also stay here longer, increasing their opportunities for repeated and prolonged exposure to additional risk factors, like sensory overload or deprivation, disrupted sleep, polypharmacy, and time.
Our next stop is the intensive care unit (ICU).
This group also skews older, a significant risk factor for delirium. People also stay here longer, increasing their opportunities for repeated and prolonged exposure to additional risk factors, like sensory overload or deprivation, disrupted sleep, polypharmacy, and time.
Our next stop is the intensive care unit (ICU).
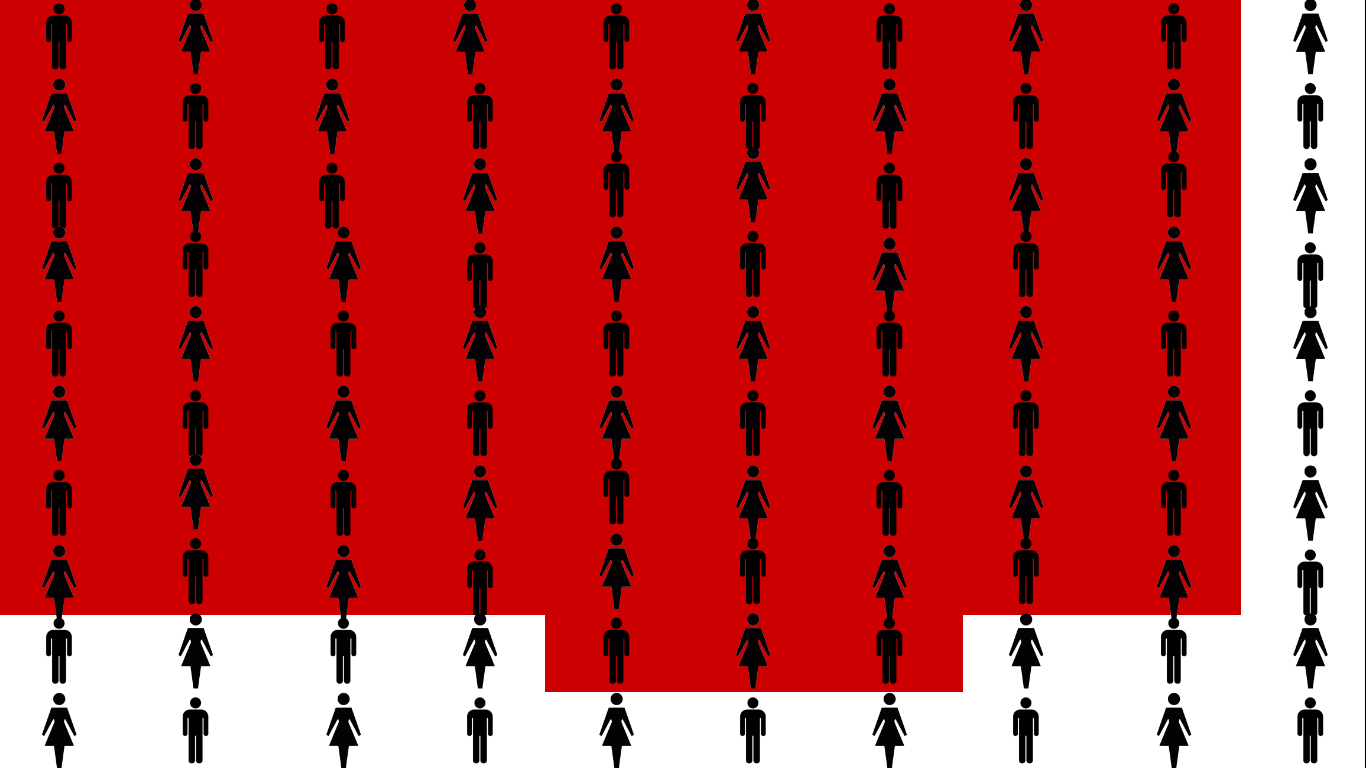
Delirium affects 75% of these, the sickest of the sick, because they’re given the most, and most powerful, medications, and are cared for in the most abnormal and disruptive setting of all.
There’s one last place for us to explore - end of life.
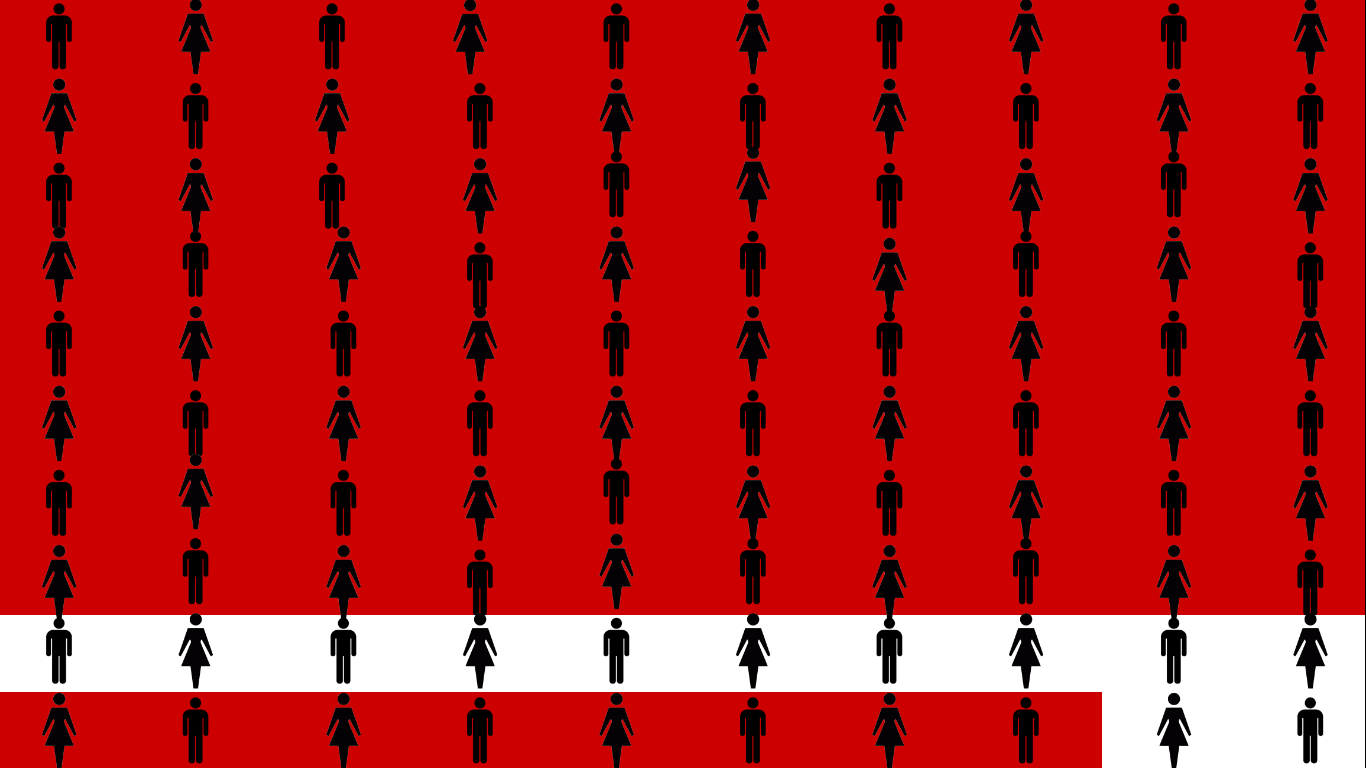
Which brings us to our Top 5 list of things every hospice clinician should know about delirium:
#5 - Expect delirium in every hospice patient. Delirium is a medical emergency. Over 85% of people at end of life experience delirium, so assume delirium is present until your assessment proves otherwise. Delirium is a deeply distressing symptom for patients and families. It undermines important goals at end of life, including comfort and meaningful interaction with family. 4, 5
***
- Inouye, S. et al. Clarifying Confusion: The Confusion Assessment Method. Annals of Internal Medicine. 1990;113:941-948.
- Andrew Teodorczuk, A. Reynish, E. Milisen, K. Improving recognition of delirium in clinical practice: a call for action. BMC Geriatrics 2012 12:55 DOI: 10.1186/1471-2318-12-55.
- Vasilevskis, E. Han, J. Hughes, C. Ely, E. Epidemiology and risk factors for delirium across hospital settings. Best Pract Res Clin Anaesthesiol. 2012 September; 26(3): 277–287. doi:10.1016/j.bpa.2012.07.003.
- Ganzini, L. Care of patients with delirium at end of life. Annals of Long Term Care. 2007;15(3)
- Szarpa, K. et al. Prodrome to delirium, a grounded theory study. Journ Hospice Palliative Nsg. 2013; 15(6):332-337.
Wednesday, April 26, 2017
What the hell, I'm gonna go with "Death Nurse."
I’m using my experience in nursing and end of life to build a business, and after much thought and several minutes with Google decided to name it, “Death Nurse.”
Well, officially, “Death Nurse, LLC,” once the lawyer finishes the paperwork.
A few of the few people I’ve told so far have been horrified, beginning with the lawyer. She said it would scare off patients and families who could be potential clients. One colleague said it played right into several bad caricatures, while another just shook her head.
The ideas at the heart of this business have been percolating in my mind for at least the past 15 years, probably longer. I’ve been a nurse for over 40 (!) years, and always worked in high-mortality settings - hemodialysis, critical care, and hospice.
In mid-career I kept my RN current while selling application software, mostly to large pathology departments at academic medical centers. I really liked working with that group of physicians.
You know, the ones who do autopsies.
My personal encounters with death started early, thanks to a culture that didn’t think twice about dragging an entire first-grade class over to the convent, to pray the rosary in French while stuffed into a tiny room with several other grades, two radiators, no windows, and a dead nun.
I value this work. I enjoy it, am challenged by it, and still learn something and/or meet someone every time I turn around.
Patients and families need more and better from us, not less: from supporting simple advance care planning and basic community education, to guiding them through overly-complex health systems - both care and financial, to helping them articulate and achieve EOL goals that really matter.
Boomers are getting old, sick, and dying. It’s a demographic wave and the surf is most definitely up.
A “good death,” however defined, doesn’t just fall from the sky. As clinicians, we need to keep expanding our knowledge and raising the bar on our practice. We’ve got to give each other the kind of care and attention we provide to patients and families.
It’s also long past time for the community to step up. Joining a walk-a-thon or donating a watercolor to the annual auction are both well-intentioned gestures, but they’re also dollar-focused and low-effort, even passive, and underscore the community’s subservience to an agency, which most agencies no doubt prefer, when power in the relationship should flow in the other direction.
I believe that the real changes we need in care, both for advanced illness and at end of life as well as for the broader system, will come from patients and families, not from us, and certainly not from any system where we might be employed.
That kind of change starts with consumers who are truly knowledgeable and able to make informed choices.
That kind of change starts with consumers who are truly knowledgeable and able to make informed choices.
At one point in my planning, a friend’s guidance led me to develop what I thought was a clever 3-step strategy to achieve this vision for a better world: Awareness, Education, and Action.
I was convinced, “If people know about x, y, z, they’ll realize the need to learn a,b,c, so they can take control and blah-blah-blah. And I can help.”
My old Uncle Ernie had a saying about revelations: “A moment to utter, a lifetime to try and probably fail.”
I’m not giving up. I’ve barely started. Some of what I’ve tried so far has gone well, some less so, some even less so, and some other still worse. There are plenty more ideas bubbling but untried, so I don’t expect many dull moments, though probably a few dead ends.
But if I’ve learned anything at all so far, it’s that it simply isn’t possible to promote awareness, education, and action without first getting people's attention.
So, yeah, I’m going with, “Death Nurse.” We’ll see what happens from there. Now I need to work on a logo and business cards.
Subscribe to:
Posts (Atom)